You may have seen the above image circulating recently and/or you may have read this article by Rick Bukata, MD. FAST-MAG was a multicenter randomized, controlled clinical trial out of UCLA studying prehospital administration of magnesium sulfate to treat stroke. The results are in.
It didn’t work.
Not necessarily surprising. This paper states we’ve tested over 20 drugs in 270 preclinical trials with ~200 clinical trials being conducted with ~40 failed neuroprotectants.
The elephant in the room is why these drugs fail to translate from the bench to the bedside. Despite success in animal studies, trials in humans have yet to work. One of the pertinent questions that was previously raised to direct the future of neuroprotectant research was that of the therapeutic window, or the time frame in which the drug should be given.
Many animal studies have been conducted with the study drug being given immediately after the onset of injury and there is usually data showing the efficacy of a neuroprotectant decreases as the time from onset increases. This is well known, however one of the translational challenges is in the marketing of the investigational drug. Pharmaceutical companies balk at the limitation of placing a ’2-hour’ time window of administration on a drug as it significantly decreases the marketability and in turn, the profitability. There is room for discussion on the role private drug companies should or should not play in clinical research. Drug companies are companies and companies exist to maximize shareholder profits. This creates a lot of pressure to find drugs which have wider administration windows than ‘immediately after a stroke’.
Enter magnesium sulfate. No drug company had a vested interest in it. There’s no patent. There’s no board of directors. There’s no shareholders. The design of FAST-MAG was to take this drug, which had no strings from the pharmaceutical industry attached, and test the 0-2 hour window. To answer the question which had been raised over and over again: Is the narrow time window the reason why neuroprotectants have failed to translate?
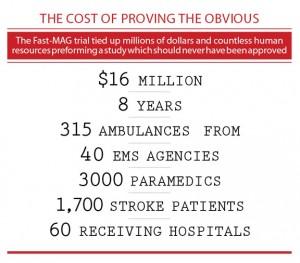
In the process a lot of data was generated and EMS agencies were thrust into the heart of clinical research. Also, a lot of money was spent: $16 million. Some feathers were ruffled in the wake hence the article by Dr. Bukata and ensuing discussion.
Open debate is always good. Science thrives on a clash of ideas and nothing should be free from rational critique. One of the goals we have with NeuroEMS is to reach out to study authors and deliver both commentary and critique from leading experts. In the wake of Dr. Bukata’s article I reached out to the principle investigators of the FAST-MAG trial for their reply. I’ve reproduced the responses received below:
Dr. Jeffrey Saver, Principal Investigator
Hi [redacted],
Thanks for contacting me. I was not previously aware of Dr. Bukata’s posting. I am ccing my co-Principal Investigator, Dr. Sidney Starkman, an Emergency Physician, and Sam Stratton, MD, and Marc Eckstein, MD, our EMS Medical Director Co-Principal Investigators, in case they wish to comment.
Here are some remarks I can offer:
The Field Administration of Stroke Therapy Magnesium (FAST-MAG) Phase 3 Trial was an innovative collaboration of prehospital, Emergency Department, and hospital systems. The FAST-MAG investigative group included 40 EMS Provider Agencies, 315 rescue ambulances, 2988 paramedics, and 60 receiving hospitals. Emergency Physicians were site PIs at each of the hospitals. The study was perhaps the largest ever undertaken by Emergency Medicine, with 715 Emergency Physician investigators, as well as 236 Neurologists, Neurosurgeon, and Hospitalist physician investigators.
The study had the specific aim of testing magnesium sulfate as a potential neuroprotective agent for stroke and the systems aim of demonstrating that prehospital start of treatment would permit delivery of therapy faster than prior ED-initiation studies, when there is the greatest potential to save threatened brain. The study succeeded in accomplishing both aims. The results on the specific aim were definitive, albeit disappointing – magnesium sulfate was not found to be a beneficial neuroprotective agent. The results on the systems aim were definitive and highly successful. Treatment initiation in the ambulance enabled start of infusion far faster than any prior stroke trial, a median of 45 minutes after stroke onset. Fully 74% of patients were treated in the first 60 minutes after onset, the golden hour in acute stroke when there is the greatest amount of brain still viable and the greatest opportunity for benefit.
As a result, the FAST-MAG collaboration has opened up a new treatment window in acute stroke, and the methods developed in the trial are already being mobilized to test many promising therapies in the pipeline, including NA-1, remote ischemic perconditioning, and hyperacute antihypertensive therapy.
I hope this is the sort of comment you were seeking. Please let me know if I can provide further information that would be helpful.
Dr. Sam Stratton, EMS Medical Director & Co-Principal Investigator
Hello [redacted],
As one of the Co-principle investigators in the FAST-MAG Trial I appreciate the opinion of Dr. Bukata, but not his lack of support for true scientific exploration of the clinical actions taken in Emergency Medicine and specifically the subpecialty of Emergency Medical Services (EMS).
The FAST-MAG trial is the model for the future scientific development of clinical practice in EMS. It appeared with early research and theory that magnesium sulfate may be beneficial as a neuro-protective agent if administered early in stroke, preferably as soon as stroke was suspected. Logically, administration in the pre-hospital setting was preferred.
Rather than adopt magnesium into the clinical practice of EMS based on early research and theory, the FAST-MAG Trial was designed to scientifically explore the intervention and was supported by NIH with no pharmaceutical company support or ability by universities to develop a new patent. FAST-MAG was the purest of science that has rarely been matched by science-like studies in almost all other area of medicine. The Trial accomplished exactly what it should have showed that adding a treatment that looked promising, had advocates, and made people feel like they were doing something to improve outcome was in fact not of the benefit expected. Without the FAST-MAG trial, the EMS community would not have the scientific evidence to address whether magnesium administration in the EMS setting for acute stroke was appropriate.
Those who fail to understand the significance of the scientific method in making evidence-based decisions also fail to understand that EMS and secondarily Emergency Medicine have progressed from following the loudest opinion to that of developing by way of true science as is illustrated by the FAST-MAG trial. FAST-MAG has raised the bar for future development of EMS and has been a study that all EMS and emergency medicine providers should be proud as being representative of the profession. For the future, FAST-MAG will serve as the ultimate example for scientific exploration in medicine.
I also reached out to Dr. Bukata and spoke with him by phone. He stood by his article as published in EPMonthly and his sentiment that the ED was the proper place to conduct the trial and not EMS.
In closing, I (Stephen) would like to offer a gentle reminder that the data should speak for itself. Boring statistics and cold, hard facts should rule the day over flashy graphics and catchy phrases. I take a bit of an issue with the image above and it was created with the intent to be retweeted, shared, and spread all throughout the world. It does not offer a rational critique of trial but rather an emotional appeal. There’s enough spin and drama in the world. Let’s conduct our scientific critiques through words not graphics which bear resemblance to the political propaganda clogging our daily news feeds. Perhaps this sounds puritanical but I think it leads to more informed discussion and less bias.
In the interest of disclosure I presently work on NIH/NINDS funded clinical research.
![]()








1 Trackback